Team:Lethbridge/HP/Gold
Human Practices (Gold)
Following our abstract exploration, we sought practical understanding of the ambulance environemnt.
Ridealongs
After completing our literature review, members of our team went on ride alongs with EMS to understand their processes better and to further our knowledge on picking the best locations to sample. We had the following objectives in mind during our ride alongs: to understand the daily cleaning techniques of the ambulances, to choose potential sampling locations, and to see first hand the types of calls that can happen in a night.

While speaking to first responders, we learned about what products they currently use to clean the ambulances. They mainly use cleaning wipes, called Caviwipes, to wipe down the ambulance after each call. These wipes are also used during monthly deep cleanings of the ambulances. Deep cleanings involve removing some equipment from the ambulance to get at areas that cannot be cleaned easily during daily cleaning. We also found out that the deep cleans occur when the ambulances are still on call.
During the calls, we looked for potential spots that could be reservoirs for pathogens based on what we saw paramedics and patients touch. Our findings were taken into consideration when narrowing down what locations we would actually sample.
The first hand experiences were also beneficial in understanding what paramedics go through each day. The calls we went on were diverse in their nature. The calls were transferring a patient to another facility, a drug overdose, and a domestic dispute.
Overall, the ride alongs helped us understand what locations would be the best to sample for potential pathogens.
Ambulance Sampling
After careful consideration of what locations were sampled in the literature, the suggestions we received from paramedics and observations from ride alongs, we chose the following areas:
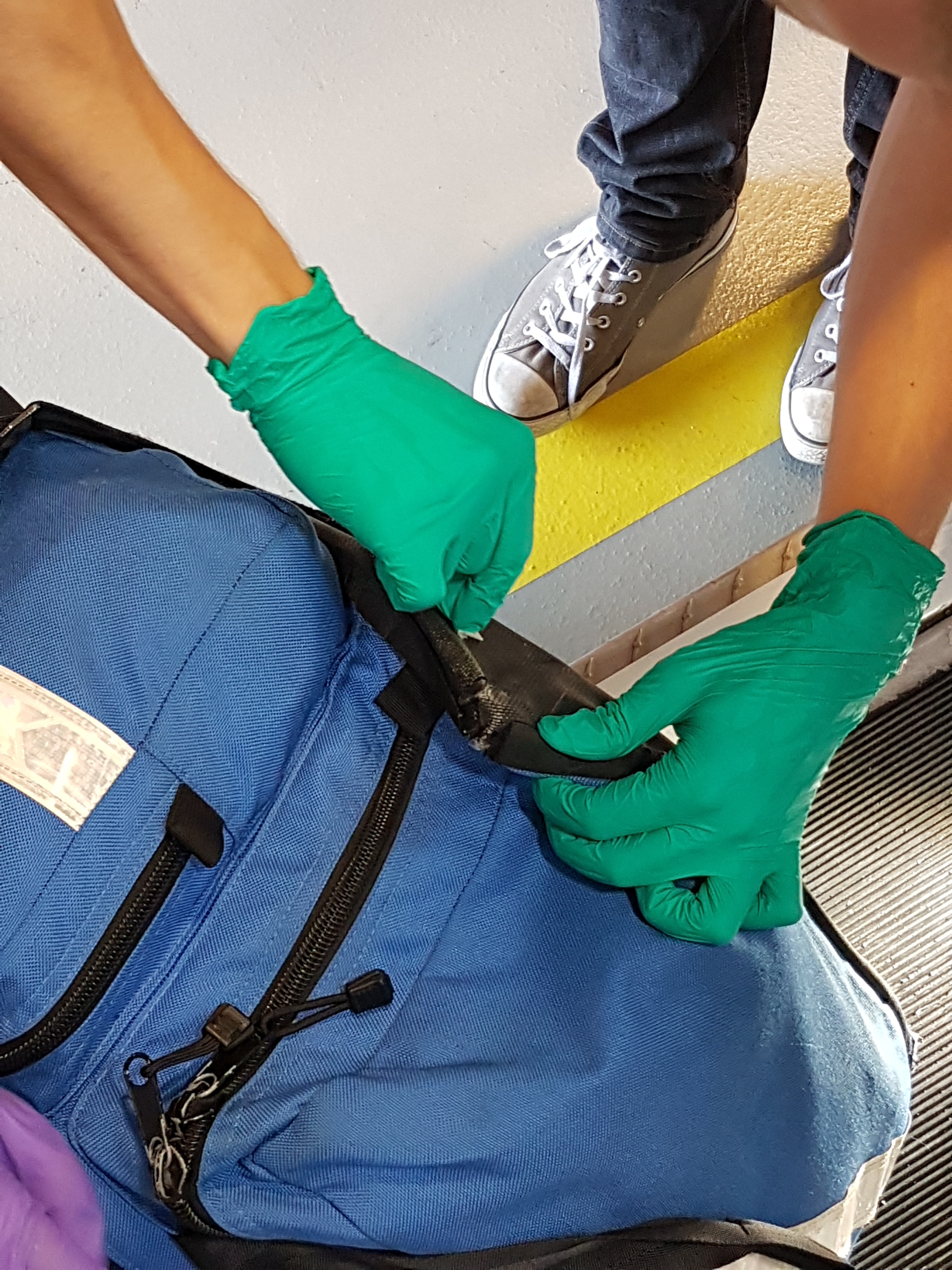
1) The bottom of a soft kit kept in the ambulance: this was chosen because it is used on every call that the EMS handle. Many of the paramedics mentioned that this might be a potential hot spot for pathogens. The bottom of this kit is made of nylon, which can trap dirt from any of the geographic locations that it is transported to. These bags are also rarely replaced because of their durability.
2) The rear back door handle: this handle is touched by the paramedics who use the ambulance throughout the day and also by some patients who are moved into the ambulance using this door. It is often the last area touched by a paramedic after moving a patient into the ambulance. Many handles were chosen as sampling locations in the literature review, such as the side door handle or handles found on the interior cupboards.

3) SPO2 finger monitor: we chose this location because patients come into direct contact with the SPO2 finger monitor, as it is needed to keep track of their vitals until they can be transferred to a health care facility. This was also another location that was mentioned by paramedics and was used as a sampling location in multiple studies we found. The paramedics did tell us that they pay careful attention to this area because of its close proximity to patients.

Protocol Design
The prevalence of virulent and multiple antibiotic resistant pathogens in healthcare facilities has resulted in ongoing reassessment of best practices to prevent their transmission. However, whether pathogen reservoirs exist in emergency medical services (EMS) vehicles, remains largely unknown. Our iGEM team developed a custom bacterial two hybrid system to select single-domain antibodies (nanobodies) that recognize human pathogens. Informed by our Nanopore next generation sequencing of DNA samples from ambulance vehicles, antibodies targeting important pathogens were then used to develop a rapid and low cost ELISA-based testing kit that may be employed on-site by EMS workers. Our project provides a framework for rapid detection of emergent pathogens and a practical and rapid solution for monitoring their presence in and outside of the healthcare system.
Prior to sampling, sample kits were prepared in house. In the biological safety cabinet, 500 L of 70% sterile ethanol was pipetted into 2 mL centrifuge tubes. ** filter paper was carefully added to each tube. The tubes were labelled, indicating the ambulance sampled, sample location and sampling week. Each kit consisted of a sterile pair of tweezers, Large KimWipes, Nitrile gloves, 70% ethanol and 12 microcentrifuge tubes (4 per ambulance).
Sampling took place at the main Fire Station in downtown Lethbridge over the course of one month. Ambulances 1, 9 and 10 were sampled every Friday at 7:00pm. All three ambulances were on call while the sampling took place.
Extra precautions were put in place in order to maintain sterility and avoid sample contamination. Nitrile gloves were worn by team members taking samples and 70% ethanol was used to sterilize gloves and the tweezers, which were used to remove the filter paper from the centrifuge tube after each location was sampled. Large KimWipes were used to dry the gloves before the next location was sampled.
The first area that was sampled was the SPO2 finger monitor located in the heart rate monitor kit. The filter paper was removed from the centrifuge tube, then the bottom part of the finger monitor that the finger is inserted into was swiped. The dimensions of this area were approximately 2 cm x 2 cm. The filter paper was then carefully placed back in the centrifuge tube.The gloves and tweezers were cleaned with ethanol between samples. This process was repeated for sampling of the rear door handle and bottom of the soft kit. The sampling area was similar in size for each location to maintain consistency throughout data collection. Following data collection, the samples were stored at -20०C until further processing.(link to experiments)
