Integrated Human Practices: iTECH
How SMITe our integrated Human Practices iTECH model has shaped SMITe and it's future as a clinical application
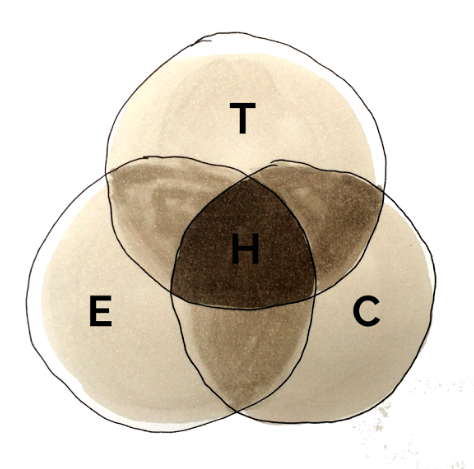
SMITe has been molded and refined by interactions between all aspects of our human practices work from the very beginning of our entry into the competition. A schematic for how the exchange of ideas has influenced our project is as follows:
Original research presented to our chosen panel of supervisors
Feedback received which focused on modifying our choice of combat proteins due to possible host immune system interactions.
Presentation of basic ideas to the Bio-hacking community of Stockholm at their annual conference- Evolving
Initial consideration of 'real life' issues: how to effectively communicate the principles of the project to the wider non-scientific community, as well as practical questions on what stage of biofilm formation to target for optimal usefulness.
Revised project plan presented at NiC- Community
Further refinement regarding best candidate combat proteins for our project and modifications to methods, based on feedback from other Nordic teams at the Mini-Jamboree. Movement away from targeting quorum sensing mechanisms.
Discussion and advice received following contact with Professor Adekile Adekunle
Guidance towards incorporation of nature’s antimicrobials, ultimately giving rise to research into defensin 1.
Inclusion and further research into defensin 1 lead to deeper consideration of world issues- Health
The increasingly-apparent need for an antimicrobial or antibiotic action incorporated into SMITe was realised; the spotlight naturally then fell on to problems posed by antibiotic resistance
Contact and discussion with clinical microbiologist further highlighted clinical consequences of antibiotic resistance- Health
Development of teaching programs related to this area -Teaching & Community
1) Teaching module for A-level students
2) Consideration that no one is too young for innovation in science: primary school project developed
Response to concerns about antibiotic resistance and it's relation to SMITe for researchers - Community
CARD system devised, further consideration of patient safety aspects discussed
Request sent to clinician in endocrinology to further explore human (patient-related) issues in continued development of SMITe -Health
Teaching:
This educational programme of case studies gave our students the basic knowledge to understand important concepts and applications in synthetic biology.
In the final months we introduced the science underpinning SMITe- which we hoped was now accessible to their understanding - and asked them to reflect on how the problem of long term wounds and the need for repeated antibiotic prescriptions are affecting us all on a global scale.
This work culminated the in addition to our Wiki of a student designed antibiotic resistance warning campaign.
Evolving:
Bio Makers: Our first public presentation of the SMITe concept occurred early in the iGEM calendar. We communicated our idea to a biology-curious cohort of members of the public at the swedish Bio-makers conference, and had the opportunity for a critique of our basic plans. This was a test of how acceptable and understandable our concept really was and gave us the valuable opportunity to seek feedback on barriers to future implementation.
Questions we were presented with included:
Where does SMITe go once it has broken down the biofilm?
Does it make the wound more wet or offensive to look at or smell bad? (or good?)
Are there actual spiders in the wound!? (This was a concerning issue for many people)
Can it be used for any wound and if not, why?
Does it hurt when it is put on open wounds?
Of course, for many of these questions we are still not far along enough in our research to be able to answer. However, it certainly gave us food for thought and made a big impact on how we communicated the concept more broadly...to avoid the worry of actual spiders being involved!
We even incorporated this into our crowdfunding campaign video...to make the issue crystal clear!
Community
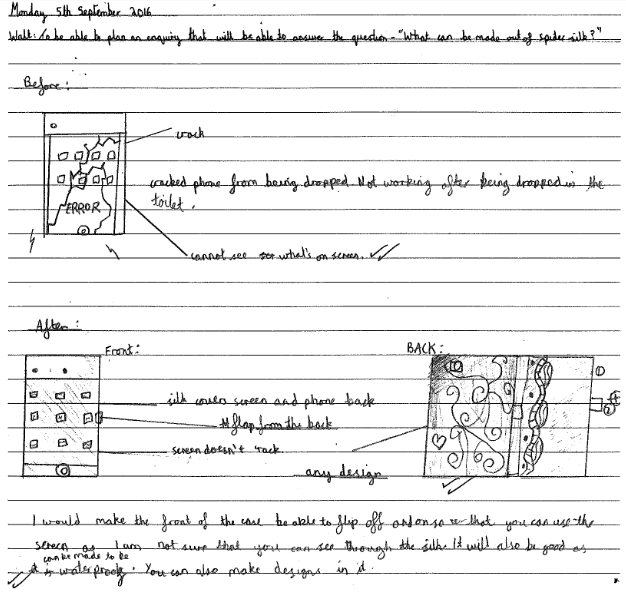
Primary school: Through our workshop based education programme, we introduced the concept of SMITe to young children at school (aged 9-11). Constituting another level of public engagement about the principles of this project, we set the task of thinking about what other purposes spider silk could serve in order to improve our daily lives. We challenged them to be as innovative and futuristic as possible... but as always when working with children, the results were surprising: several examples are shown below. (The final part of the web resource was a short video about a scientist who had trialed human skin samples reinforced with spider silk and demonstrated they could be bullet proof...I think this struck a cord with the students!)
Protecting an iPhone
 A helmet cover- for reinforcing the protection offered by helmets for soldiers
A helmet cover- for reinforcing the protection offered by helmets for soldiers
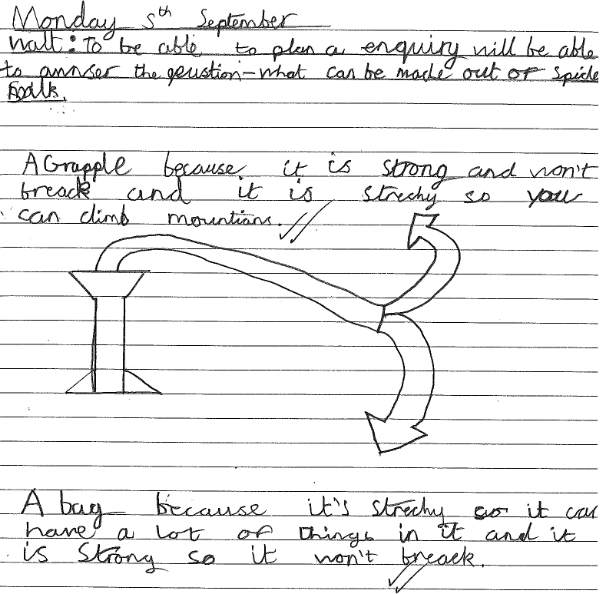
 A grapple rope as spider silk is so strong!
A grapple rope as spider silk is so strong!
CARD system:
Health
Interview: With insights from Professor Rotimi's research into chronic wounds, we continued to model our focus on s.aureus biofilms. This provided us with a framework which was both safe and accessible for us to work with in the lab as well as being clinically relevant to the problem. Our reflections on the interview with Professor Rotimi resulted in a mindset-shift towards the rapidly emerging problem of antibiotic resistance. Although we had originally concentrated on chronic wounds as a considerable economic healthcare burden that impacts the lives of vulnerable patients in terms of morbidity, this interview really opened up our outlook. We considered how the current therapeutic options for these wounds is actually a driving force to the problem of antibiotic resistance, and considered the issues of continued pressure to combine our new approach with drugs we already know are losing ground in the battle against bacteria.
From this interview we also learned to differentiate colonised from wounds which are secondarily infected. We considered how SMITe could easily have a role in the management of poorly healing wounds which were still vulnerable to infection, but with no systemic features. Since the early biofilm production (especially in diabetic wounds) originates from s. aureus, perhaps SMITe could have an even greater role in preventing secondary infections than treating them "once the anaerobes have moved in."
In response to this, we discussed the problem with our panel of supervisors and took advice about the incorporation of an antibacterial instead of an antibiotic into the SMITe. We were encouraged that this might be possible, but unfortunately did not have time to be able to develop and adapt the idea further (so far).
Furthermore, we considered the possible consequences of releasing previously stagnant bacteria from a biofilm into the local wound environment, but also to face the immune system and possibly systemic circulation of the individual being treated.
Again, we are currently far from the point of needing to worry about these issues, as the foundations of our idea are still emerging. However, we concluded that there are a number of possible outcomes:
1) Bacteremia- serious and better avoided but with the advantage that bacteria could now be targeted through intravenous antibiotics...rather than festering in a wound and dormantly developing resistance following attempts to clear wounds with systemic treatment
2) Successful immune clearance of the bacteria and rapid healing of the wound (ideal)
3) Unknown effects!
Ethical Approval:
Professor Rotimi introduced the concept of seeking ethical approval to trial SMITe, with the concern that coupling it with an antibiotic could promote the risks of resistance.
However, we considered further reaching complications of ethical approval and whether SMITe as a novel concept has more benefits to offer than risks.
How could you conduct ethically acceptable trials, not knowing what this structure might do? This issue is of paramount importance in trialing all drug candidates, so we respond to this question by intending to follow safety and toxicity testing protocols and working from the ground up in terms of in vitro, in vivo and clinical trials. We feel it could offer a possible low risk therapy for individuals who have tried all else and have life or limb threatening wounds.
Is the concept really new? We know already that not many biological wound dressings are in use but spider silk use in wounds dates back centuries, as it was observed to be non-immunogenic.
As a treatment platform however, our SMITe structure has many benefits to offer over the silk itself, including the futuristic possibility of constituting a personalised medication.
Could it be possible that in the future we could all attend a doctor's surgery, have our wound "read & imaged" in terms of it's microbiology and landscape, and a personalised SMITe dressing synthesised there and then!
This is based on the thought that if spider silk can be coupled with s.aureus combat proteins...why not others?
Could SMITe be applicable in a clinical setting? With the caveat of passing safety testing and toxicity trials- why not?
Is it acceptable in principle to patients to have a dressing of this nature? If maggots are an acceptable option, we think this is more benign, as possibly preferable if it is successful.
Could it be cost effective? As with any new, novel concept in therapeutics, recouping expenses is a necessity. However, with the added benefits of avoiding protracted inpatient stays for surgical debridement and dressings if it were to be effective, an appropriate but higher price than conventional dressings might turn out to be cost saving. Additionally, any new treatment able to provide an alternative to repeated antibiotics is an important weapon against this global threat and is therefore worth it's weight in gold!