Difference between revisions of "Team:TAS Taipei/Modeling"
(Undo revision 115969 by Averyw17113532 (talk)) |
|||
| Line 15: | Line 15: | ||
background: #f3f4f4;} | background: #f3f4f4;} | ||
| − | + | p{font-family: Lato !important;} | |
} | } | ||
Revision as of 07:46, 10 September 2016


Modeling
Overall Modeling Abstract
Our goal is simple: produce GSR/25HC, package it into nanoparticles, and transport into the lens. GSR/25HC is released over time, which decreases H2O2 concentration, reduces crystallin damage, and prevents cataracts. Our models approach these steps in reverse order, starting with our desired goal, and working backwards to understand the entire process.
In model 1, we quantified crystallin damage, and measured its true impact on light absorbance, to relate it to cataracts. Then in model 2 we modelled how varying amounts of GSR added impacted the amount of crystallin damage, until we found a desirable GSR level for cataract prevention. We examined the degradation of nanoparticles in model 3, and how repeated doses in the long-term contributed to sustain the desirable GSR level. Model 4 accounts for the actual transport of nanoparticles into the highly protected eye, mainly by flooding the eyedrops with GSR so sufficient amounts entered the eyes. Finally, Model 5 is a simple stochastic model for understanding gene expression in a simple circuit.
Outline

Introduction
Why Model?
In the lab, biologists are often unable to test everything experimentally. For example, in our cataracts project, cataract prevention occurs in the long-term, from 20-50 years. Obviously, although short experiments can provide us an idea of what prevention may look like, the power of computational biology allows us to model into the future. As a result, our modeling has been crucial in developing a prototype.
Focus
Most iGEM teams perform modeling on gene expression, which we accomplish in model 5. However, as our construct is not directly placed into the eyes, how our synthesized protein impacts the eyes after it is seperately transported is much more interesting. As a result, we spent the majority of our models on understanding the impacts on the eye.
Guiding Questions
- How much GSR do we want inside the lens?
- How do we use nanoparticles to control the amount of GSR in the lens?
- How do we synthesize GSR, package into NP, and send it into the eye?
Model 1: Crystallin Damage
Abstract
An absorbance measurement is meaningless without knowing how clinically severe it is. Cataract severity is graded on the LOCS scale from 0-6, and our goal is to lower LOCS to 2.0, below the threshold of surgery. We relate measurements made on different scales, from LOCS to opacity, light transmittance, light transmittance, wavelength absorbance, and finally to crystallin damage, a quantity that is useful for our future models.
Purpose
What amount of crystallin damage is acceptable, to not require surgery? This will let us know how much GSR we need to maintain an acceptable amount of crystallin damage that will not require surgery (based on LOCS scale)
Conclusion
To make sure LOCS rating remains under 2.5, which has equivalent absorbance value of 0.108 a.u, we must add enough GSR to decrease crystallin damage until it is below 1.941 M-h.
To make sure LOCS rating remains under 1.0, which has equivalent absorbance value of 0.0299 a.u., we must add enough GSR to decrease crystallin damage until it is below 1.220 M-h.
Model 2: GSR/H2O2
Abstract
Abstract
Purpose
Purpose
Conclusion
Conclusion
Model 3: Nanoparticles
Abstract
Abstract
Purpose
Purpose
Conclusion
Conclusion
Model 4: Eyedrops
Abstract
Abstract
Purpose
Purpose
Conclusion
Conclusion
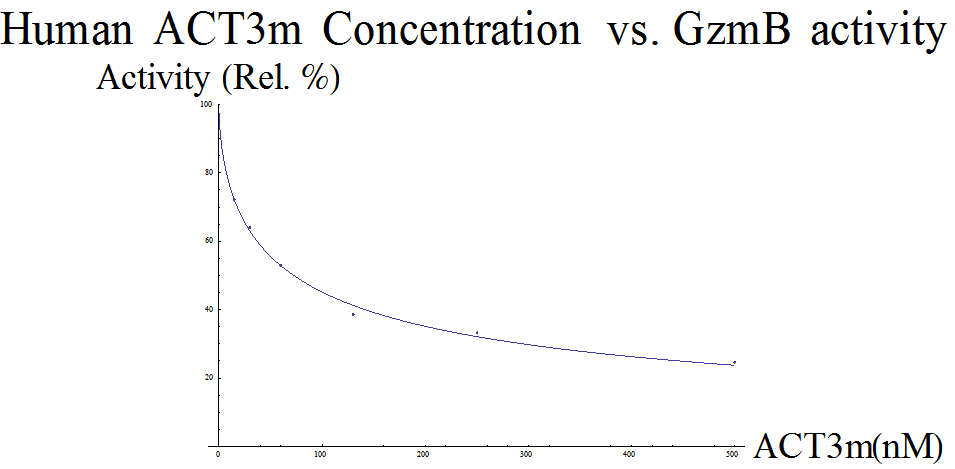
Human GzmB Inhibitor ACT3m
HOME
Given our model of Serpina3n, we also wanted to create a model for the protein used in our device, ACT3m. The dataset obtained from the ACT3m paper (Marcet-Palacios et al., 2014) is the result of a colorimetric assay. Data was presented as absorbance values (A405), which correspond to the concentration of free GzmB, at different inhibitor concentrations. The paper used this to prove that their novel ACT3m inhibitor was the strongest out of their entire pool of possible candidates: treatment with ACT3m resulted in the lowest A405 values, which suggests the strongest inhibition of GzmB.
Menu 1
To model this set of data, similar adjustments had to be made. First, the dataset was scaled so the numbers ranged between 0 and 1 (in this case, increased by a factor of 2). The same modified Hill equation was used from the Serpina3n analysis. Our model returned a Kd of ≈ 13.336 and n ≈ 0.605, so the equation looks like  (Figure 2).
(Figure 2).
Menu 2
Conclusion
Yay
Citations
